Patient: What was my blood pressure at my last visit?
Doctor: That’s part of your medical record. I’d rather not say.
Sounds absurd, right? It is. And I’m guessing not many doctors have had that attitude. But prior to Congress passing the Health Insurance Portability and Accountability Act (HIPAA) in 1996, there was no federal law requiring health care practitioners to give you access to your own medical records or information. (Some states did have a law to that effect, though.) Now that access is guaranteed – even if you haven’t paid your bill – although practitioners are allowed to charge a “reasonable” amount for providing the information.
As more and more practitioners and facilities transition to electronic health records, some are piloting a new type of on-demand access: electronic patient portals. While they differ some in format or the extent of information available, the idea is that the portal is a secure, online repository of your medical information, from physician notes, to medication lists, to lab or test results, to upcoming visit schedules, and so on. These portals are often also interactive, allowing patients to schedule appointments, message their practitioners, and request medication refills.
Rush University Medical Center, which my internist is affiliated with, offers “MyChart,” its own patient portal system. There never seemed to be much reason to view it, though. After my recent run-in with the medical establishment, I decided to check it out, more for curiosity than anything.

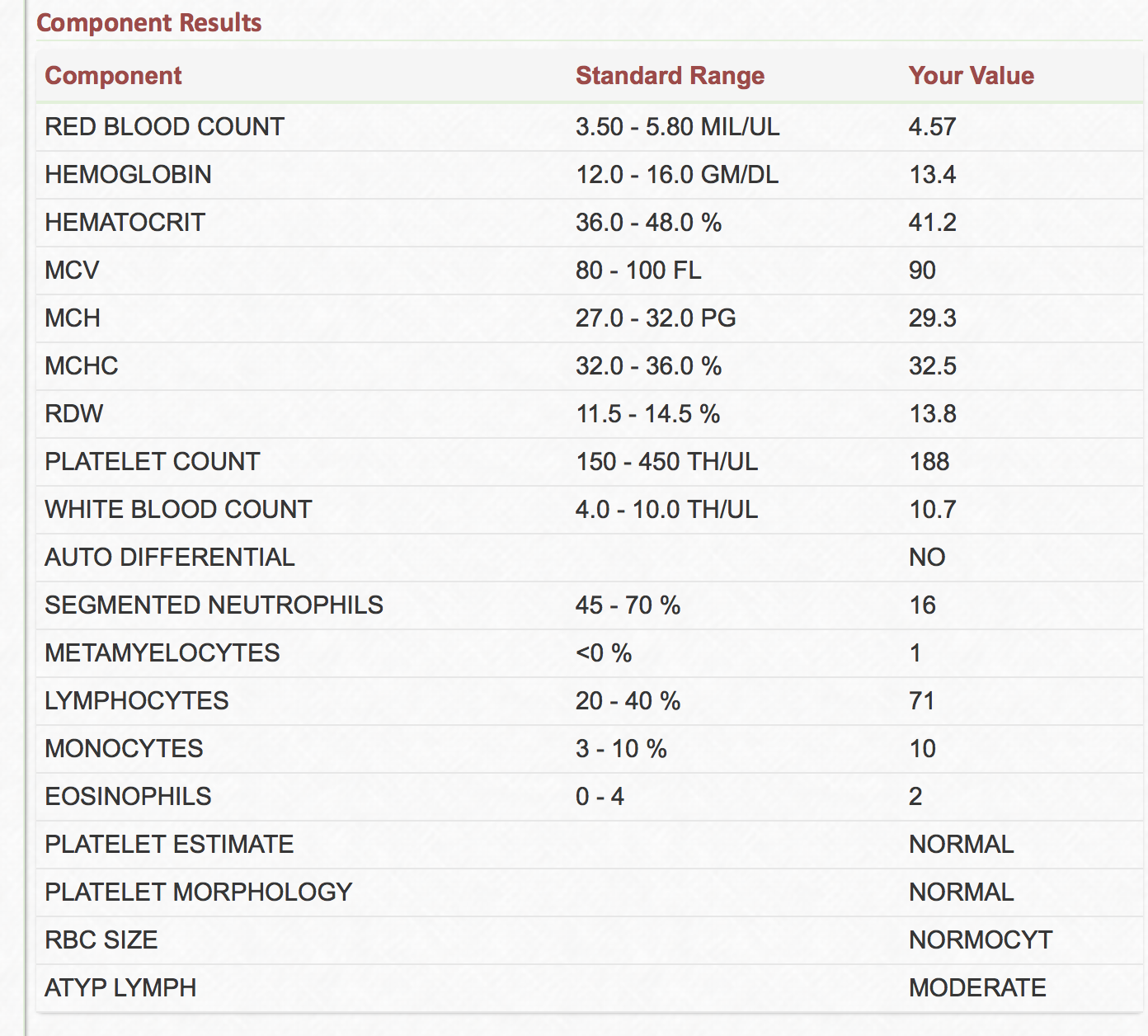
Through the MyChart patient portal, I have access to a wealth of medical information, including these lab values.
It’s really pretty cool (at least for a curious pre-medical student such as myself; its efficacy for the general public is still a matter of debate; more on that later). For example, I was able to view all my labs from when I was in the ER, everything from my mono test (positive) to my strep culture (negative) to all of my CBC values. Upon opening up the CBC link, for example, two columns appear – both the standard ranges and my values.
OK, I’m no doctor (yet). So when I see values outside the normal range, or narrative values that make no sense to me, I have the tendency to become curious (at the least). For example, what the heck does “ATYP LYMPH / MODERATE” (at the very bottom of the screenshot) mean? Enter my good friend Google: this signifies that my immune system is actively fighting an infection. One Web site I found even specifically referenced infectious mononucleosis, explaining that mono produces a lymphocyte morphology with a dented cytoplasm, in addition to some other specific characteristics. So. I’ve got dented lymphocytes. Who knew?
So far, my use of MyChart has really been more for curiosity’s sake than anything, though. The true purpose of an electronic patient portal is to better patient outcomes, increase transparency in health care, improve coordination and continuity of care, enhance practitioner-patient communication, and foster a sense of ownership regarding one’s care (among other things). The question is: do patient portals live up to these goals?
To answer this particular query, I turned to another dear online friend, PubMed.* While my search on the subject is by no means exhaustive (or particularly scientific), here is a theme I found repeated:
We don’t know yet.
In fancier, more scientific language:
Evidence is mixed about the effect of portals on patient outcomes and satisfaction, although they may be more effective when used with case management. The effect of portals on utilization and efficiency is unclear, although patient race and ethcnicity, education level or literacy, and degree of comorbid conditions may influence use.
[Source: “Electronic Patient Portals: Evidence on Health Outcomes, Satisfaction, Efficiency, and Attitudes,” Annals of Internal Medicine, 2013]
Like I said.
The reason we don’t yet know how beneficial patient portals are is that they are relatively new, which means studies on them lack the longitudinality, detail, and context necessary to make convincing conclusions. The review article quoted above mentioned that in the studies they looked at, patient attitudes regarding the portals are “generally positive.” On the other hand, it seemed that not all patients had equal access to or understanding of the information available: “… more widespread use may require efforts to overcome racial, ethnic, and literacy barriers.” In other words, it becomes a health literacy issue, one complicated by the involvement of technology.
The review article’s bottom line:
Portals represent a new technology with benefits that are still unclear. Better understanding requires studies that include details about context, implementation factors, and cost.
That said, there is anecdotal evidence that patient portals are a positive development. Another article in the Annals of Internal Medicine, from 2012, looked at a group of 105 primary care doctors who provided electronic links of their visit notes to some 13,564 patients across three different practice sites. The self-identified goal of the study was to “evaluate the effect on doctors and patients of giving patient access to notes over secure Internet portals.”
The overarching result of the study:
At the end of the experimental period, 99% of patients wanted open notes to continue and no doctor elected to stop.
[Source: “Inviting Patients to Read Their Doctors’ Notes: A Quasi-Experimental Study and a Look Ahead,” Annals of Internal Medicine, 2012]
More detailed statistical findings, summarized below, were quite interesting as well (statistical ranges are given to represent the differences between practice sites).
Of the 5,391 patients who opened at least 1 note and completed a postintervention survey:
- 77% to 87% across the three sites reported that the open notes helped them feel more in control of their care
- 60% to 78% of those taking medications reported increased medication adherence
- 26% to 36% had privacy concerns
- 1% to 8% reported that the notes caused confusion, worry, or offense
- 20% to 42% reported sharing the notes with others
After the intervention, the physicians were surveyed as well:
- 0% to 5% reported longer visits
- 0% to 8% reported more time addressing patients’ questions outside of visits
- 3% to 36% of doctors reported changing documentation content
- 0% to 21% reported taking more time writing notes
This anecdotal study has both strengths and weaknesses. A strength, and something I appreciate as a future physician, is that the authors did survey the doctors as well – important because anytime you introduce something new like this, you need the doctors on board to make it work. Making conclusions from this study, though, is dicey. The authors acknowledge this upfront with a “Limitations” section at the top of the paper: Only three geographic areas were studied. Most patients were already experienced in using such portals. Both doctors and patients choosing to participate and complete the final survey “may tend to offer favorable feedback.” The end survey response rate was low (41%).
Still, the results are something to think about. If, somehow, we could develop strategies for overcoming the racial, ethnic, and literacy barriers (as cited by the first review article), then maybe we could see more of these positive results across the general population.
Or … maybe not. But if it might help people take ownership of their health, I think it’s worth a try.
* In case you’re not familir with PubMed, it is basically a ginormous collection of scientific and medical journal articles online, curated by the US National Library of Medicine and the National Institues of Health. Some of them are free; others are available for purchase on the specific journal’s Web site. Being a Northwestern University employee, though, I have access to most of the articles at no charge. Gotta love connections.