Flashcards: Prokaryotes
Another set of flashcards for this Friday’s bio exam … this one also has some cool pictures, so check it out!

A sample of my flashcards from this deck on Quizlet.com.
Another set of flashcards for this Friday’s bio exam … this one also has some cool pictures, so check it out!
A sample of my flashcards from this deck on Quizlet.com.
I’ve got a big biology exam coming up this Friday (March 4), so in preparation I’ve been making more flashcards. Here is a set on cladistics. I will also post sets on prokaryotes and protists. If any of you out there are in my class, hope this helps!
– Lorien

Sample of my flashcards from this deck on Quizlet.com.
Last December, I tried out a fun Facebook app called “My Top Words of 2010.” It (supposedly) went through all my status posts from the year and came up with a list of the words I used the most. My top word? PHYSICS. (I used it 11 times, in case you’re interested.)
For those of you who have been following this blog for some time, or who know me personally, this should not be a surprise. It’s not that I don’t like physics. I actually find it quite interesting. But I also find it quite difficult.
Case in point: the homework we were assigned to do a couple of weeks ago on electric fields and point charges took me at least 6 hours to do, if not more (and 2 of those hours were spent at a tutoring session). I understood it by the end, but it took a lot of work. And a lot of help. (Which, by now, I’m not afraid to ask for.)
A week and a half ago, we had our first exam of the semester. Prior to that, my professor handed out a set of 49 (that’s right, 1 fewer than 50) optional practice problems. Doing well on these physics exams is not so much about being able to solve the problems, but being able to solve them quickly. And the only way to build up speed is to practice, practice, practice. So, being the dedicated (and slightly insane) student I am, I did every one of those practice problems. All 49 of them. For several days leading up to that exam, I went to bed thinking about physics problems, and I woke up thinking about physics problems. I breathed physics problems.
Come exam day, though, I still felt unprepared. After my professor handed out the test, I looked at the first problem and blanked out. Knowing that I had no time to waste (we had 7 multiple-part problems to do in 50 minutes), I skipped it and moved on to a problem I could quickly do. I worked to the end of the exam and finally circled back to that first problem. I answered it as best I could and handed in my test at exactly the 50-minute mark. Done. Thank god.
As the adrenaline wore off, my mood plummeted. I had felt rushed the whole time and was sure my answers were riddled with stupid errors.
Well, I got the exam back Tuesday afternoon: 93%. Mine was one of four As between both physics sections (about 40 people total). The class average was in the 70s.
I talked for a few minutes with my professor about the exam, and he said he was able to tell from his post at the front of the classroom who had done the practice problems and who hadn’t. He said he could tell I was one of the few who really knew what I was doing because I worked through the problems quickly, without hesitation. (Which was a bit funny, considering I sure didn’t feel I knew what I was doing!)
It’s clearly a confidence issue for me. And one I don’t have in my other classes: biology and chemistry exams don’t fill me with the same kind of dread, nor do I leave them thinking that I flunked.
I have pondered this a great deal, and here is what I have come up with: physics is out of my “comfort zone,” if that makes sense. It’s not the kind of science that I’m used to, and it involves a very different way of thinking about the world. (Literally.) So I have this niggling doubt that perhaps, maybe, I won’t be able to “get” it. Which, of course, I’ve proven wrong to myself over and over. (I got a high A last semester, and have an A so far this semester as well).
I really see taking physics as an important learning experience for me. And I’m not talking about the material, although that is obviously necessary for doing well on the MCAT. What I’m talking about is developing a different attitude and approach toward material that perhaps isn’t my strength. Not fearing it, but embracing it as a challenge, and still retaining confidence that if I put my mind to it, I will succeed. Obviously, I haven’t quite grasped this concept yet … but I’m working on it.
I had a fantastic journalism professor in college who told us it was our job as journalists to be uncomfortable, to step out of our comfort zones and learn and experience something new. Well, I’m no longer a journalist, but that professor’s advice still holds true: you really do learn something about the world, and about yourself, when you put yourself in that kind of situation.
In short: you grow. And isn’t that what life is all about?
In a previous post, I mentioned that I had found a great iPhone / iPad app called Flashcards++, which allows you to create digital flashcards and import them to your Apple device and study on the go. (Always a good thing for us busy students!) You can both make the flashcards directly on your iPhone / iPad, or make them on one of two Web sites (Quizlet.com or Flashcardexchange.com) and then import them. I use Quizlet.com. I discovered yesterday that I can “embed” the flashcards in my blog. So I thought that I would do that and share a bit of what I’ve been studying: Mendelian genetics. (That, among many other things!) Feel free to flip through the flashcards if you like. It’s kinda fun, in a really nerdy and geeky way. But then again, if you’re going into medicine, you have to embrace that inner nerd, right? RIGHT?! Enjoy.
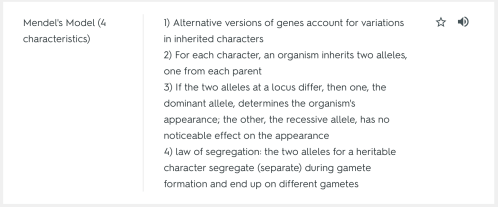
A sample of my flashcards from this deck on Quizlet.com.
While translating this week at the free clinic where I volunteer, I helped out with two back-to-back intake appointments. “Intake” meaning brand new patients to the clinic, and meaning the medical practitioner had to take an entire medical and social history before getting down to what was bothering the patient that day. I had translated for intakes before, but never back-to-back ones. Working with them in such high concentration really got me thinking about the importance of taking a good medical history: how it very often provides the tools for making a more complete diagnosis and understanding what is going on physically, and psychologically, with a patient. And how without it, you would be lost.
The first patient, a middle-aged woman, came in with wrist pain. Suspecting tendonitis or carpal tunnel, the doctor asked whether the woman had ever worked in anything where she did repetitive motion. Turns out she used to work with jewelry. Turns out she also had surgery on her other wrist for carpal tunnel many years back. Bingo! The doctor then prescribed anti-inflammatory medication to try and relieve the symptoms, with the hopes that the patient wouldn’t need another surgery. Had the physician not known about the patient’s past, it would likely have taken much longer to make a diagnosis and to find something to bring the patient relief.
A nurse practitioner saw the second patient, a younger woman with rheumatoid arthritis who had been taking a high dose of steroids to relieve her arthritis pain. When it came time to do a “review of systems” — to check her health (literally) from head to toe — she responded with a “yes” when asked if she had a problem with nearly every area mentioned. Headaches, blurry vision, the list went on. It became quite clear that it was the long history of taking steroids that was likely causing all of these problems. The solution? Taper off the steroids and start another arthritis-relieving medication. Again, had the nurse practitioner not asked very detailed questions about her medication history (which he did), there is no way he would have known that her problems were a result of the steroids, and no way he would have been able to (hopefully) resolve the situation.
There are so many things you need to know about a patient, so many things that could affect their well-being. So many questions, many of which may not be pertinent to one patient, but may make the difference for another patient’s treatment. For example, if you know someone has a family history of diabetes, you can keep closer tabs on their sugar levels, and also impress on them the importance of eating right, exercising, etc. Not that you wouldn’t do that for every patient — but you could emphasize that there is added risk because of the family history. And that might help convince them to take their health more seriously.
Listening to the physician and the nurse practitioner take those medical histories gave me a better sense of what I will need to do when I become a doctor. It was good experience for me to be exposed to not only what questions to ask, but how to ask them: with compassion and sensitivity (especially the more delicate questions). Luckily, as a former journalist, I am an experienced interviewer. So I have that going for me. What I am learning is a new set of questions, and how to interpret a new set of answers.
“A second federal judge ruled on Monday that it was unconstitutional for Congress to enact a health care law that required Americans to obtain commercial insurance, evening the score at 2 to 2 in the lower courts as conflicting opinions begin their path to the Supreme Court.”
– from the New York Times (click on the link for the whole article)
The provision in President Obama’s health care bill referenced in the above quotation is set to go into effect in 2014. Republican-appointed Judge Roger Vinson, who made the ruling, also found the rest of the health care bill unconstitutional. The whole matter is surely destined for the U.S. Supreme Court, as the Times article suggests.
I don’t pretend to be a constitutional scholar. So I don’t feel I can comment on the “constitutionality” of the health care bill, nor on the specific provision requiring all Americans to purchase commercial insurance. Nor do I want to get into a debate regarding party politics. Those of you who know me know where I stand politically, and this blog post is by no means a political party statement. So don’t even go there.
That said, I have an opinion on the efficacy of the health care insurance provision, based on my own experiences working in the medical field.
First of all, I believe all Americans deserve proper health care. In our convoluted health care system, that means (most likely) having insurance of some sort, be it individually-purchased insurance, or government-provided insurance. But forcing people to buy insurance on their own dime is another matter. Here is why I think that is a problem.
I work at a free clinic in Chicago where the only requirement to be a patient is that you have absolutely no insurance. That means no private insurance, no Medicare, no Medicaid. This clinic is for the people who fall through the cracks: the people who can’t afford insurance on their own and who don’t qualify for government assistance, either because they are undocumented immigrants or because they don’t meet the income “poverty” requirements the government sets forth. I don’t know exactly how many patients the clinic has, but I do know that the extensive filing system in the clinic’s office is full to bursting, and that doctors and nurse practitioners do new intake appointments every day. There is clearly a need for this type of service in the Chicago community.
But these people, who are people, let’s not forget, not numbers, nor statistics on a chart, do not come to this clinic by choice. They are there because they need this service. Because many of them can barely afford the basic necessities of daily living, such as food, electricity, the bus fare to get to work (if they are lucky enough to have a job — probably a minimum wage one — at all).
Asking them, nay forcing them to buy health insurance (or face a penalty), is forcing many of them to give up something else that they desperately need. Food, electricity, the bus fare to get to work. The list goes on.
While the government is planning to expand Medicaid eligibility (according to the same NY Times article), I doubt very much whether that supposed “safety net” will safely catch all of these people.
This provision of the health care bill is well intentioned, I understand that. It is meant to make sure that people receive health care when they need it, and don’t wind up with enormous out-of-pocket expenses when some horrible illness strikes. The formation of “health care exchanges” is also meant to drive down rates for people who have to purchase insurance on their own. Those are obviously good goals, and I support them.
But what has not been taken into account is that there are scores of people who literally cannot afford even $25 a month per person in their family for health insurance. I have met many of them. And I cannot, in good conscience, support such a provision.
Constitutional? I have no idea. Conscientious? Not according to my experience in the real world. And that, I believe, is what many politicians lack: real-world experience. Or at the least, they are so far removed from it that they have forgotten what it’s like out there in the real world. And that’s just plain sad.

During medical school, I hope to go abroad for at least one international medical rotation.
It’s important to get in to medical school, obviously. But it’s also important to fit in to a medical school. Because you will be there for four years. A tough four years. That means thinking about what kinds of criteria are important to you (or in this case, me) as a potential medical student.
I’ve done some thinking about this. And while I haven’t come up with an exhaustive list, I have developed some ideas on what I am looking for. If I developed these criteria in one blog post, it would be rather onerous to read, so I have decided to divide this into a series of posts. (At least, that’s the plan.)
So how do I know what I want? Figuring that out involves knowing myself pretty well. Which is one benefit of being a “non-traditional” (translate: older) student. I’ve had more life experiences — and time — to learn about myself, what works for me, and a little bit more about what I want out of life. I have a much better idea of these things than I did 10, or even five, years ago.
One characteristic I am looking for in a medical school is the opportunity to do at least one international rotation as a medical student. That means going abroad during my time as a medical student (typically during the third or fourth year, when I would actually have some clinical skills) and working in a clinic or hospital in that foreign country.
Why would I want to do such a thing? After spending a semester abroad in Chile while I was an undergraduate student, I realized the importance of gaining exposure to other cultures, other languages, other people, other ideas. Not that I hadn’t thought that was important before — but its importance was impressed upon me more than ever. Being in Chile was, by far, the best experience of my undergrad education. I think everyone should study abroad, if at all possible. It was an invaluable educational experience — not so much in the classroom, as out in the streets of Chile, Peru, Bolivia, and Argentina.
Of course, I would love to hit those same street again — this time as a third- or fourth-year medical student (or resident) — but I would also be interested in seeing other parts of the world.
Fortunately for me (and others), the Association of American Medical Colleges (AAMC) and Foundation for Advancement of International Medical Education and Research (FAIMER) have put together an online database of medical schools that offer such opportunities, called “International Opportunities in Medical Education,” or IOME. Click here to visit the database.
According to a basic search I did on that database, 74 medical schools offer international opportunities to their own students (you can also search for resident opportunities, faculty opportunities, etc.).
That’s pretty amazing. And I can’t wait.
A couple of weeks ago when I left the free clinic where I volunteer as a Spanish medical translator, I thought to myself, “I belong here. And I like that.”
Not that I hadn’t had this feeling of belonging before — but it has definitely cemented over the last few shifts I’ve worked.
On a basic level, part of it is knowing my way around the neighborhood — the quickest route to the clinic, where to find parking even during rush hour, what drink to order at the local cafe when I need a caffeine boost.
There’s also something to be said for now being on a first-name basis with the clinic coordinators and the volunteer coordinator, and being known as someone who can be relied upon to come through when the clinic is especially short-staffed.
My Spanish — which was excellent to begin with — has improved as well, which helps me feel more comfortable in my role as an interpreter for the patients, doctors, nurses, and other medical practitioners.
My Spanish skills were particularly tested, and mostly affirmed, recently. (Although I was also dealt a bit of humility in the process.)
Typically, I translate for primary care appointments — medication refills, diabetes check-ups, pap smears (a papanicolaou, in Spanish — try saying that 10 times fast!), that sort of thing. This appointment was a little different. The practicioner was a registered dietitian, and the patient was there to get some tips on how to eat healthier and lose weight. Which is knowledge many of us take for granted. But, as I learned, is knowledge that is very cultural in nature.
Juan* was from Ecuador, and had been in the United States for about 15 years. He had put on 30 or so pounds in the last few years, partly as a result of American food — a few too many hamburguesas at McDonald’s, he said. He had developed severe sleep apnea, which required surgery. His doctor said he needed to lose weight before having the operation. So he was quite motivated to get in better shape.
But he had no idea where to begin. And he had a lot of misconceptions about healthy eating and weight loss that needed challenging and changing.
“Whenever I go on a diet,” he said, “My stomach acts up. So how can I go on a diet?”
It turned out that to Juan, going on a diet meant eating puras frutas y verduras — all fruits and vegetables — which would make anyone’s stomach unhappy. Not to mention that it’s unhealthy, because you’re not getting balanced meals.
So far so good, as my Spanish was concerned. Then things got tricky. The dietitian started explaining the chemical mechanisms as to why eating a balanced meal is important — you need protein at every meal so that your body doesn’t start to digest your muscles. That was certainly something I’d never translated before! And you need fiber to help pass the food along in your system. To my embarrassment, I translated that as: Necesita fiebre para ayudar en pasar la comida por su sistema. Juan looked really confused for a moment. Then clarity hit him. Quiere decir fibra, he said. Oops. I’d been saying “fever” instead of “fiber.” Luckily, we both got a good laugh out of it. So did the dietitian.
Aside from my fever-fiber faux pas, I seemed to be able to get everything else across. Juan asked question after question, wanting to understand every little detail of how to proceed. “I want to know what to do so that when I get home, I’m not confused,” he explained.
I was impressed with his motivation and dedication. This man knew next to nothing about healthy eating, and he wasn’t afraid to admit it. On the contrary, he brought up every question he could think of — including plenty that to those of us who grew up learning about the food groups and the need for balanced nutrition, might seem ridiculous. “One of my friends told me that if you drink water right after you eat, your stomach gets fat. Is that right?” he asked. The dietitian patiently explained that no, you can drink water whenever you want to, that it actually helps with digestion. Juan soaked it all up like a sponge.
The dietitian had prepared a week’s worth of meal plans for Juan, and we spent a lot of time going over that, as well as determining correct portion size. I reached back into the past, to my high school days, trying to recall all the food vocabulary I’d learned back then. To my (pleasant) surprise, it came back, for the most part.
There was so much information to translate (I kept having to stop the dietitian so I could remember what he had said and make sure to translate it all), so much different vocabulary from what I usually translate in an appointment, so many explanations that I’d never had to make before. But the satisfaction of seeing how much Juan learned, and how excited he was to now have these tools, was so worth it.
I don’t know how Juan is doing. Obviously, it’s up to him whether he will use the tools he has acquired. But truly, knowledge is power. And I feel so honored that I had even a small part in helping him gain that power.
*Name and some details have been changed to protect patient privacy.
I’m not normally one to endorse particular products or brands. Because as a rule, I hate advertising. So I avoid inflicting it on others.
But when it comes to Apple, I bend my own rules. I write this (and every other) blog post from my trusty MacBook Pro, which I absolutely adore. I own not one, not two, but three iPod devices (a regular iPod, an iPod touch, and an iPhone). And when the iPad 2 release is announced — rumored to happen this quarter — I will be first in line to pre-order my own, as I mentioned in a previous post.
Why? Of course there are games, music, movies, all that jazz. But really, and I mean this sincerely, I want to use it as an educational and practical tool. I call it my “iEducation.” Let me explain, by way of introducing some of the apps (that’s short for “applications,” for those of you less familiar with the smart phone and iPad frenzy) I plan to get.
 Flashcards++ (Jason Lustig, $3.99)
Flashcards++ (Jason Lustig, $3.99)
I already own the iPhone version of this app, and it’s fantastic. For anyone who uses flashcards, I highly recommend it. (FYI – there are a bunch of flashcard apps out there, and I combed through them all and decided this was the best for my purposes.) You can make flashcards directly on your iPhone (or iPad). Or you can make them on the Internet (which I find easier) and import them to your Apple device. Then once you’ve imported the cards, all you do is tap the screen to flip them over. There are study modes and test modes, and the program keeps track of your score (you punch in whether you got the card “right”) so you can monitor your study progress. Flashcards++ supports the use of two different flashcard Web sites, www.Quizlet.com and www.Flashcardexchange.com. I’ve been mostly using Quizlet; I prefer its interface. With Quizlet, for $10 more a year, you can use images on your flashcards — a feature I’ve found to be worth its weight in 3x5s. But not only can you make your own flashcards, you can search through literally thousands of other people’s flashcards and import them as your own. Everything from art history to biology to French. I personally find that making the flashcards helps me retain the information, but everyone learns differently.
MCAT Review (Watermelon Express, $19.99)
I won’t be taking the dreaded MCAT for more than a year. But there’s no time like the present to start studying. And while there are better-known MCAT review programs out there — including one by Kaplan — this is the highest-rated one, and the one that seems to have the best content. Watermelon Express sells its physics, chemistry, and biology MCAT study apps separately, but if you buy them together in this package, you save $10. Sounds good to me.
 Instapaper (Marco Arment, $4.99)
Instapaper (Marco Arment, $4.99)
This app allows you to save Web pages — i.e., newspaper, magazine, or journal articles — for later (offline) reading. The really cool thing is that it saves them as text pages, which “optimizes for the iPhone and iPad screens,” according to the iTunes store site. With all the scientific journal articles I’ve been reading lately, this would be quite handy.
 iAnnotate PDF (Aji, LLC, $9.99)
iAnnotate PDF (Aji, LLC, $9.99)
Speaking of scientific journal articles … one of the main reasons I want to get an iPad is to that I have a convenient, portable way of reading all those long articles without having to print them out. But I need to be able to highlight them, write notes in the margins, circle important figures, etc. This app allows you to do just that. And it’s gotten rave reviews.
 Penultimate
Penultimate
(Cocoa Box Design LLC, $0.99)
Handwriting notes on the iPad. How cool is that? Draw pictures, sketches, chemical compounds, whatever. You organize your various pages in “notebooks” of your choosing (infinite notebooks are available). You can also send your pages to anyone in PDF form. Pretty nifty.
Quickoffice Connect Mobile Suite
(Quickoffice, Inc., $14.99)
While I much prefer the Mac OS, let’s face it: most documents we use these days are in Microsoft format (Word, Excel, etc.). This app allows you to open, edit, and create those types of documents on the iPad.
dPad HTML Editor (drikin.com, $6.99)
Clearly, I enjoy blogging. But if I could do more with HTML, I could do more with my blog. I’m hoping this app will allow me to do that.
And this is only the beginning …
P.S. My username on Quizlet.com is “menhenne” if anyone wants to check out my own flashcards. Mitosis, genetics, molecular bonding … good stuff.

Tropical cocktail with a 3-D protein structure as a garnish. My kind of beverage.
It was like a two-person game of telephone. You know, the childhood game where one person whispers something in a person’s ear (“I ate pizza for dinner”) and the next person hears something totally different (“I hate Lisa Windsor”) and it gets passed along until the beginning phrase is no longer recognizable. Silliness usually ensues. This time was no different.
My mom and I were talking (and we were actually on the phone). I told her I had been searching for some protein research topic on PubMed (the National Institutes of Health online article database). After I had been talking for a few moments about the articles I found, she burst into laughter.
“I was really confused there for a second,” she said. “I thought you said ‘Club Med,’ not ‘PubMed.’ ”
I started laughing too. But then I thought about it. Maybe she had something there. And somehow my dream vacation took form over the phone — in the union between Club Med and PubMed.
Picture this: a giant cruise ship sailing in the Caribbean. Swimming pools, tennis courts, a fancy restaurant and bar. Stops at various islands for exploring, shopping, hiking, beachcombing, fishing, etc. But this is no ordinary cruise ship, nor an ordinary cruise crowd. On board is a fully equipped, world-class research lab and a mini convention center. Those aboard the cruise are scientists interested in protein research, and they have come together to collaborate on research and present their latest findings at a floating scientific conference.
Since my mom helped me come up with the idea, I wholeheartedly agreed that she could be my “plus-one” at the conference. She said that sounded great, as long as she could bring a drink into the conference room. Fine by me, as long as the drinks have edible 3-dimensional protein conformations as garnishes. And as long as the drinks are named after proteins.
Tom cholinesterase, anyone?
